|
Patients may undergo functional endoscopic sinus surgery under intravenous sedation and local anesthesia or under general anesthesia. The authors' institutional preference is general anesthesia. The procedure begins with decongestion of the nose and infiltration of lidocaine with epinephrine (1% lidocaine with 1:100,000 epinephrine is used for injection). The lateral nasal wall near the uncinate process is injected. Using a 3-mL syringe while placing a slight bend to the 27-gauge needle facilitates the injection. Next, the superior inlet and the anterior face of the middle turbinate are injected submucosally. If the possibility of septoplasty exists, the septum should also be injected. Next, 4 mL of 4% cocaine is placed onto pledgets, which are placed bilaterally in the nares. A throat pack may be placed, or, alternatively, the stomach may be suctioned prior to extubation upon completion of the procedure. The patient is then draped for surgery. If image-guided surgery is to be used, the appropriate headset apparatus should be applied at this time. Functional endoscopic sinus surgery may begin with uncinectomy. If the uncinate process can be initially visualized without manipulating the middle turbinate, uncinectomy can be performed directly. Otherwise, the middle turbinate is gently medialized, carefully using the curved portion of the Freer elevator to avoid mucosal injury to the turbinate and to avoid forceful medialization and fracture of the turbinate. Next, uncinectomy may be performed via an incision with either the sharp end of the Freer elevator or a sickle knife. The incision should be placed at the most anterior portion of the uncinate process, which is softer on palpation in comparison to the firmer lacrimal bone, where the nasolacrimal duct is located. Then, a Blakesley forceps is used to grasp the free uncinate edge and to remove it. Complete uncinectomy is important for subsequent visualization. Incomplete uncinectomy is a common reason for failure with primary surgery. The backbiter may also be directly used to take down the uncinate process. Once the uncinate process is taken down, the true natural ostium of the maxillary sinus should be identified. The protected eye may be palpated at this juncture to ensure no dehiscence of the lamina papyracea and to confirm the location of the lamina. The natural ostium is typically at the level of the inferior edge of the middle turbinate about one third of the way back. A true cutting instrument is used to circumferentially enlarge the natural ostium. The optimal diameter for the maxillary antrostomy is controversial; typically, a diameter of 1 cm allows for adequate outflow and for postoperative monitoring in the office. Care should always be taken to avoid penetrating the lamina papyracea. Next, the ethmoid bulla should be identified and opened. A J-shaped curette may be used to open the bulla at its interior and medial aspect. Once the cell is entered, the bony portions may be carefully removed using a microdebrider or a true-cutting forceps. Complete resection of the lateral bulla facilitates proper visualization and dissection posteriorly. Again, care should be taken laterally to maintain an intact lamina papyracea. The remainder of the anterior ethmoid cells may be uncapped initially with a J curette and further opened with a microdebrider or a true cutting forceps. Using a curette initially allows for tactile sensation and determination of the thickness of bone and verifies proper orientation prior to further opening of cells with powered instrumentation. Care should always be taken to avoid mucosal stripping because mucosal preservation results in superior postoperative outcomes. Anterior ethmoid cells should be cleared to the skull base, with the surgeon exercising caution when approaching the ethmoid roof and maintaining constant reference both to the endoscopic view and to the preoperative CT scan. Image-guided surgery or computer-aided surgery also guides the surgeon as to the distance to the skull base, but it does not replace the need for an intimate knowledge of the anatomy. While moving posteriorly to new air cells, the surgeon should always enter inferiorly and medially and then subsequently open laterally and superiorly once the more distal anatomy can be judged by visualization and palpation. Anterior ethmoidectomy is complete upon reaching the basal lamella of the middle turbinate.
If the sinus disease is limited to the anterior ethmoid cells and the maxillary sinus, the procedure may end with simple anterior ethmoidectomy and maxillary antrostomy. If, however, significant radiographic and clinical posterior ethmoid and sphenoid disease is present, then dissection should continue to exenterate the posterior ethmoid cells and to perform adequate sphenoidotomy as appropriate.
Posterior ethmoidectomy begins with perforating the basal lamella just superior and lateral to the junction of the vertical and horizontal segments of the middle turbinate. Care must be taken to preserve the posterior sagittal section of the middle turbinate and the inferior portion of the coronal segment of the basal lamella. By preserving this L-shaped strut, the stability of the middle turbinate is ensured. The lateral and superior portions of the basal lamella may then be removed using the microdebrider. Further posterior ethmoid cells may be taken down in a similar fashion, keeping in mind the location of the skull base and the lamina. The surgeon must be cognizant that the skull base typically slopes inferior at an approximately 30° angle from anterior to posterior. Thus, the skull base lies lower posteriorly than anteriorly. This dissection is taken back to the face of the sphenoid.
In the absence of Onodi cells, the sphenoid ostium lies medial and posterior to the final posterior ethmoid cell. A rough guide is that the face of the sphenoid is approximately 7 cm from the nasal sill at a 30° angle from the horizontal. Identifying the superior turbinate aids in the confirmation of position. The sphenoid sinus is entered just medial and inferior to its natural ostium with a J curette or an olive-tipped suction. Once the sinus is entered safely, the ostium can be enlarged using a mushroom punch forceps. Care must be taken not to aggressively enter the sinus because dehiscences may be present in the bony coverage of the carotid artery or the optic nerve.
Frontal sinus work is typically reserved for the end of the surgical procedure because manipulation may create bleeding and obscure further posterior work. If frontal sinus work is indicated, a 45° or a 70° telescope proves useful. Typically, an agger nasi or frontal cell is the cause of frontal outflow obstruction. Using an angled scope for visualization, a frontal sinus curette is passed above the cell and then pulled anteriorly, thus breaking posterior and superior cell walls. Particular care must be exercised when working in the frontal recess because both the lamina and the skull base sit in immediate proximity to the outflow tract. Image-guided and navigational systems for computer-aided surgery and intimate knowledge of the anatomy are critical for safe frontal sinus work. For further discussion of endoscopic frontal sinus surgery, see the text by Kuhn and Javer.
Once dissection is complete and hemostasis is achieved, a bacitracin-coated Telfa pack is placed into the nostril. This packing is removed prior to discharge of the patient. The patient is discharged with Ocean Nasal Mist and antibiotics, as well as instructions for a follow-up visit in 1 week. Some surgeons also place Gelfilm within the middle meatus to keep the space open and to prevent lateralization of the middle turbinate and synechiae formation. If placed, Gelfilm should be removed on the first postoperative visit.
| |
COMPLICATIONS |
Section 7 of 10    |
|
|
All risks and benefits should be candidly discussed with patients as part of the informed consent process prior to surgery. A patient should never undergo surgery without a full discussion of all possible complications.
Risks associated with endoscopic sinus surgery are as follows:
- Bleeding
- Synechiae formation
- Orbital injury
- Diplopia
- Orbital hematoma
- Blindness
- CSF leak
- Direct brain injury
- Nasolacrimal duct injury/epiphora
| |
OUTCOME AND PROGNOSIS |
Section 8 of 10 |
|
|
Outstanding short- and long-term results have been reported. In one study, symptoms improved in 66 of 72 patients following endoscopic sinus surgery, with a mean follow-up time of 7.8 years (Senior, 1998). In another report, quality of life improved for 85% of the patient population, with a mean follow-up time of 31.7 months (Damm, 2002).
| |
FUTURE AND CONTROVERSIES |
Section 9 of 10 |
|
|
The realm of endoscopic surgery is continually being expanded. Procedures that were traditionally performed using external incisions are now being performed endoscopically. In some clinical settings, inverting papilloma excisions and limited skull base tumors are being approached endoscopically. Early results with these procedures are promising, but long-term outcomes regarding recurrence and success rates are only beginning to be reported in the literature. Further study is required to delineate the role of endoscopic surgery in those areas.
Pearls of wisdom regarding endoscopic sinus surgery are as follows:
- When entering each new space or landmark (eg, bulla ethmoidalis, anterior ethmoid cells, basal lamella, posterior ethmoid cells, sphenoid), the safest location for entry is medial and inferior.
- The patient's CT scan should be examined preoperatively for location of the skull base on coronal cuts.
- Frontal recess is best evaluated on sagittal CT sections.
- The uncinate process most often attaches to the lamina papyracea superiorly, thus leaving the frontal recess to drain medially and superiorly to the uncinate.
- The sphenopalatine foramen and the sphenopalatine artery are adjacent to the lateral and inferior attachment of the basal lamella to the lamina papyracea.
- Orbital hematoma/postoperative proptosis requires immediate removal of nasal packing, emergent ophthalmologic consultation, and emergent lateral canthotomy.
Fess For Paediatric Rhinosinusitis
Introduction:
Sinusitis in the pediatric population has become a common diagnosis in the last 10 years. The definition of Sinusitis in general terms is the inflammation of the lining of the paranasal sinuses. Acute sinusitis most often manifests as a complication of viral upper respiratory tract infection of which a child averages 6 to 8 per year. It is estimated that 5 to 13% of children experience sinusitis.
Sinusitis is classified on the basis of duration. It can be acute (duration less than 30 days), subacute (2-3 months), or chronic (more than 2-3 months). Acute sinusitis is most likely infectious where as chronic may be a combination of infectious and noninfectious.
The primary therapy for the pediatric patient with sinusitis is medical. In the case in which the sinusitis is recalcitrant to maximal medical management or they develop complications the role of functional endoscopic sinus surgery has evolved. This is still a controversial area and it will be reviewed.
Development/Embryology:
The sinus develop during gestation as four paired paranasal invaginations of the nasal cavity. The maxillary sinus are the first of the human paranasal sinuses to develop. This begins as a bud along the inferolateral surface of the ethmoid at around gestational day 65. The ethmoid cells develop during the third and fourth fetal months as evagination of the lateral nasal wall in the middle meatus region. The ethmoid and maxillary sinuses are pneumatized soon after birth. The sphenoid sinus originates during the third fetal month as a paired evagination in the sphenoethmoidal recess. The sphenoid sinuses are pneumatized at approximately age 3. Embryologically the frontal sinus starts to envaginate from the anterior ethmoid cells at 4 months gestation and are pneumatized by age 6.
Radiographically the maxillary and ethmoid sinuses are evident in early infancy, the frontal sinus become evident at age 6 and the sphenoid by age 8.
The development of the nose and paranasal sinuses after birth are directly linked with the development of the facial part of the skull and dentition. The structures of the anterior ethmoid and middle meatus; like the uncinate process, ethmoid infundibulum, hiatus semilunaris and bulla ethmoidalis are thought to be well developed in the newborn. They are used as constant anatomical landmarks.
Pathophysiology:
As we know the sinuses are made up of four sinuses: paired maxillary, paired ethmoid, frontal and sphenoid sinuses. The nasal cavity contains three turbinates for humidification of the air. They have significant expansive capacity. The posterior ethmoid cells and sphenoid sinuses drain into the superior meatus. The maxillary, frontal, and anterior ethmoid sinuses drain into the middle meatus, which contains the osteomeatal complex.
There are three conditions which are necessary for the sinuses to function normally. These are a patent ostia, normal mucociliary function and normal quality and quantity of secretions. Impairment of any combination of these three conditions can lead to chronic or recurrent sinus disease.
The conditions that contribute to obstruction of the ostia can be divided into two classes: mechanical and systemic. The mechanical obstruction comes from polyps, synechia, deviated nasal septum, turbinate hypertrophy, inflammatory edema or nasal tumor. The inflammatory edema is probably the most common and is usually the result of upper respiratory tract infections or inhalant allergy. The second function mentioned is normal mucociliary function which can be altered by viral infection and primary ciliary dyskinesis. This leads to inadequate clearance of secretions leading to ostial obstruction. The allergic inflammatory disease which is regulated through IgE- mediated release of histamine results in mucosal edema and increased production of nasal secretions. Now if you have a disorder in one or more of these three functions and then introduce a pathogen, sinusitis will develop. There are also a few systemic illness in children that make them prone to developing sinusitis. Some well known conditions are cystic fibrosis, immune disorders, primary ciliary dyskinesia, immotile cilia syndrome and cyanotic heart disease.
There are also some who suggest the existence of a noninfectious sinusitis. The inflammation is a noninfectious response involving numerous inflammatory cells which are responsible for the release of mediators capable of damage in the mucosal integrity.
Microbiology:
Most pediatric sinusitis develop after viral upper respiratory tract infections. The are usually superinfected with a bacterial pathogen. The pathogens in acute childhood sinusitis are the same as those described in adults: Streptococcus pneumoniae, non typable Hemophilus influenzae, and Moraxella catarrhalis and Staphylococcus aureus. They are also the same pathogens as in Acute otitis media linking the two infections together. Studies that have suggested a role for organisms like coagulase negative staphylococci, other alpha-hemolytic (non-pneumococcal) streptococci, propionibacterium and corynebacterium species, and various anaerobes have only demonstrated the sensitivity of their culture techniques in isolating skin and oral normal flora. Most pediatric texts remark that Streptococcus pneumoniae, Hemophilus influenzae, and Moraxella catarrhalis (in high numbers) are normal flora in a young child. It is common (60% of two year olds), but not normal since these children have the symptoms of sinusitis.
Chronic sinusitis has a predominantly anaerobic flora. Most commonly anaerobic gram-positive cocci, staphylococci and streptococci, with occassional bacteroides. The aerobes are culture 35 % of the time with Hemophilus less prevalent than with acute infections.
Diagnosis:
Sinusitis is a common pediatric diagnosis. It can be acute or if persistent for more than 3 months be classified as chronic disease. It is estimated that 0.5-5% of upper respiratory tract infections are complicated by acute sinusitis. The majority of these episodes resolve spontaneously, resolve with antihistamine and decongestant therapy, or require only a single course of antibiotics. Compounding the issue is that 10 to 15% of the children experience seasonal or perennial allergic rhinitis by 16 years of age.
The diagnosis of pediatric sinusitis has went through significant changes in the last 10 years. There is still much controversy in the diagnosis of chronic sinusitis and recurring sinusitis. The emphasis must be placed on history and physical examination. In especially younger children the symptoms and the radiologic findings may be quite confusing. The diagnosis should be based on a combination of clinical history, findings on the physical examination, laboratory results and the radiologic findings. The younger the child the more nonspecific the findings compared to older children and adolescents whose symptoms more parallel adults.
The most common symptoms in young children is rhinorrhea both anterior and posterior(77%), otitis media(66%) and cough(48%). Malodorous breath is also common. A frequently missed finding is morning periorbital edema. The symptoms which are common to adults such as headache, facial pain and fever are much less common in children. Sinusitis commonly follows and upper respiratory infection and respiratory allergies.
With recurrent sinusitis the presence of inadequate initial therapy must be taken into account or the presence of systemic and local factors. The recurrence of 3 episodes in 6 months or 4-5 episodes in a year require more extensive clinical evaluation. They can have local factors such as polyps, deviated septum, foreign body or allergic problems. If the patient has host-defense mechanism, then one would also anticipate other sites of infection such as recurrent otitis or infections involving the lower respiratory tract. Patients with serum and secretory IgA deficiency, the most common immunoglobulin deficiency, have a history of recurrent sinopulmonary infections. This also seen with patients with functional antibody deficiency syndromes with IgG subclasses may manifest as recurrent acute and chronic sinusitis. Kartagener's syndrome with immotile cilia syndrome have frequent sinus problems and are often diagnosed with electron microscopy of the cilia.
Chronic sinusitis persists for greater that 3 months. Patients have similar symptoms to acute sinusitis except more constant nasal discharge or posterior nasopharyngeal secretions manifesting as chronic nasopharyngitis. These patients develop suborbital venous congestion, the so called ocular "shiners." Otitis media and asthma are often related to chronic sinusitis. Again local and systemic reasons can be the cause.
Evaluation:
The most common clinical scenario is the persistence of the signs and symptoms of the upper respiratory tract infection beyond the typical 7 to 10 days without overt improvement. Symptoms noted do not allow distinction of acute viral infection of the upper respiratory tract from sinusitis because no single symptom is specific for the diagnosis of sinusitis.
A peripheral blood white cell count and the differential and sedimentation rates are usually of no clinical value. Nasal smears are thought to be of some value. They will have a large number of PMN especially with intracellular bacteria. One must be aware of the high number of PMNs present in a simple viral infection. The presence of mucopurulent material in the middle meatus is confirmative of the diagnosis of acute sinusitis. Nasal and throat cultures correlate poorly with cultures of sinus aspirates. Because of the invasive nature of aspiration of the sinuses, it is not routinely used for the diagnosis of acute childhood sinusitis.
Plain radiography is the most common method used by the pediatrician for the diagnosis of acute sinusitis. In comparison with the CT scan these two methods in chronic childhood sinusitis has lead to questioning of the efficacy of plain radiography for the diagnosis of this condition. The correlation is good between total opacification and air-fluid levels of the maxillary sinuses on plain films and CT. The ethmoid are unidentifiable on plain radiography and will not be picked up on plain films. Plain films do allow sinusitis to be identified but the amount of disease is hard to quantitate. Another problem with plain radiography is the different criteria used by radiologist as being diseased. Various degrees of mucosal thickening (2-6 mm), opacification, or air- fluid levels have all been used as criteria for diagnosis. Underdeveloped sinuses may be misinterpreted as being opacified. Air fluid levels are frequently not present since uncooperative children often necessitate the film to be taken in a supine position. There is often a lack of correlation between symptoms and radiologic findings.
In children with a recent or current infection of the upper respiratory tract without signs and symptoms of acute infection have a high frequency of abnormalities on plain films. The reverse is also often seen when the child is very symptomatic and normal films will be present. It has been found that plain radiographs are unreliable in children younger than 1 year of age. However for the pediatrician plain films are helpful in the diagnosis of acute sinusitis when it is unclear or as a method to follow resolution or unresponsiveness to therapy. But if the results from the history and physical examination are strongly suggestive it is reasonable to forego plain radiography and proceed with treatment. The plain film is nonsensitive and possibly non- specific imaging media for evaluation of the young child with sinusitis.
Of limited usefulness is sinus transillumination, ultrasound and endoscopic examination (in younger children.)
CT scans are the "gold standard" for the establishment of sinusitis. But the CT scan must be critically evaluated. It may be to sensitive in demonstrating virally-mediated and "post-infectious (residual or resolving) inflammatory" changes in the sinuses. There is an impressive radiographic lag ( 6 - 12 weeks) in clearing of the sinuses, after microbiologic and clinical cure occurs as seen in adult studies. Now if you superimpose the multiple viral infections that children have nearly all children will have some sort of abnormality on CT. The CT is a just a "snap-shot in time."
Potential surgical candidates must have axial and coronal CT scan. The CT scan must be of good quality because even slight variations from normal are critical. The CT scan must be coronal cuts of 3-4 mm with appropriate bone windows. The CT scan demonstrated pathologic variations and the ever critical ostiomeatal complex. The imaging should be performed only after intensive medical management if symptoms persist or complications develop.
The findings usually underestimate the findings seen in the operating room. Occasionally the patient with definite symptoms and clinical picture of sinusitis with minimal disease one CT may still benefit from surgery. The CT scan usually does not indicate frontal sinus disease even though this is usually prominent feature in children with inadequate treatment.
Cystic fibrosis children are a unique situation. They have been found to have a unique feature on CT scan. The patients had medial displacement of the lateral nasal wall in the middle meatus and uncinate process demineralization.
Nasal endoscopy is difficult to perform on children adding to the difficulty in diagnosis and the post operative care. The uses of Medazolam (.25mg) instilled intranasally in most children allow endoscopic examination.
The decision to perform surgery usually is made on the basis of the combined diagnostic criteria of appropriate symptoms, physical examination findings, and CT imaging results.
Therapy:
In acute sinusitis therapy can be approached in two ways. The first approach is to treat patients with amoxicillin for 10 to 14 days. It an initial 2 week period of therapy fails, an additional course of a beta lactamase resistant antibiotic (such as a second- generation cephalosporin or Augmentum) should be started. A second approach is based on the increasing number of Beta-lactamase-producing organisms. A considerable number of H. influenzae and M. catarrhalis organisms have been reported to produce beta lactamase in acute sinusitis. This treatment includes initial management with a beta lactamase resistant antibiotic for 7 to 10 days beyond resolution of symptoms. This will usually be a duration of 2 to 3 weeks. Additional treatments with topically applied or orally administered decongestants, isotonic saline nose drops, spray or irrigation, steroid inhalants, antihistamines, and topically applied or orally administered anti-inflammatory medications.
Decongestants are thought to increase ostial patency yet has questionable impedance on mucociliary clearance. The saline irrigation and steam treatments appear to have only anecdotal benefits. Supposedly, therapeutic benefit is due to moisturizing the inflamed mucosa and softening the nasal crusts. Antihistamines are only considered with concomitant allergy due to the interference in clearance of secretions by thickening the mucous. Inhaled steroids are often used as adjuncts to treatment of sinusitis especially if component of nasal allergy. If symptoms persist or worsen 48 to 72 hours after the initiation of the antibiotic treatment, the patient should be re-examined and future test run to rule out complications. Operations are rarely indicated in acute sinusitis unless there is a complication or is in conjunction with underlying chronic sinusitis. It has been found that seizure disorders and asthmatics have a decrease in attacks with the treatment of sinusitis.
FUNCTIONAL ENDOSCOPIC SINUS SURGERY (FESS):
The major operative differences in children are the anatomic size of the surgical area and the extent of pneumatization of the individual paranasal sinuses involved in the disease process.
Patients in whom conservative therapy including maximal medical therapy, adenoidectomy, and allergy treatments have failed and continue to have frequent recurrent or chronic episodes of sinusitis are candidates for FESS. The conservative FESS technique dictates that the extent of the procedure performed be proportional to the extent of the disease present. Mucus membrane disease in children is frequently limited to the ostiomeatal complex (omc). Children with even more extensive disease seem to resolve with the restoration of adequate ventilation and drainage to the OMC area.
The use of functional endoscopic sinus surgery is often better than the conventional approaches. Children must have maximal medical management for an extended period of time even before FESS is contemplated. The child should have extensive documentation the sinusitis is truly recalcitrant to optimal therapy.
To prevent postoperative complications all children must be screened for factors that suggest hematologic abnormalities, recent ASA or ibuprofen intake. The most common cause of FESS complications is poor visibility secondary to excessive bleeding.
The "mini FESS" is the best approach to acute and chronic pediatric sinusitis. All children procedures are performed under general anesthesia. The positioning of the patient is important. The child fovea ethmoidalis and cribriform should be at 90 degrees from the table and the head straight forward. This is an important safeguard and helps avoid penetration of these structures. It is also recommended that the surgeon sit at a 90 degree angle to the patient.
The surgical requirements in children are much more exacting than in adults. Only special pediatric operative instruments should be used. The 2.7 mm telescope with a high-intensity light source should be available, especially to start the case.
The injection is performed with lidocaine with 1:100,000 epinephrine. Care must be taken to limit the injection to no more than 7 mg/kg. The injection is placed into the greater palatine foramen and root of the middle turbinate. The maximal safe dose of lidocaine/epinephrine is according to weight and only the proper amount should be available on the surgical set up. After the injection pledgets soaked in oxymetazoline are placed in the middle meatus. Cocaine is rarely used in a child less than 16 due to its cardiac side effects.
The steps are the removal of the lower portion of the uncinate process followed by the creation of a middle meatus antrostomy using the natural ostium of the maxillary sinus and then inspection of the interior mucosa of the bulla ethmoidalis.
The floor of the maxillary sinus is not necessarily at the level of the floor of the nasal cavity, care must be taken in surgery directed at the maxillary sinus prior to age eight. The use of inferior meatal antrostomies should be avoided for functional and also anatomical reasons. There are risk to the tooth buds and the spongiotic bone under the floor of the sinuses.
The uncinate process is taken down from lateral to medial using a back biter. The sickle knife is not used since it makes cuts medial to lateral risking the lacrimal system and the orbit. The inferior turbinate may be located high up on the lateral nasal wall, resulting in the uncinate process being in closer proximity to the papyraceous lamina. Many times a ball tipped seeker is used first to place within the infundibulum to minimally displace the uncinate anterior medially which will assist in getting the back biter in place. The OMC is then found within 1 to 2 mm of the anterior uncinate as it inserts into the lateral nasal wall. The natural ostium is almost always in the most anterior and superior portion of the fontanelle. If residual lower uncinate is left in place this frequently causes obstruction and the need for revision.
There are three "pearls" for verifying the natural maxillary sinus ostia:
- 1. The natural ostia do not lied in the same plane as the lateral nasal wall. Their anterior lips are more lateral than the posterior lips; that is, they lie in the oblique plane.
- 2. Accessory ostia tend to be perfectly circular, whereas the natural ostia are a variant of oval.
- 3. The natural ostia are almost always anterior and or superior to accessory ostia.
The most common cause of FESS failure is opening the middle meatus antrostomy that is not in continuity with the natural ostium. The purulence that escapes through this diseased drainage pathway then reenters the ineffective but larger accessory ostium, a phenomenon called recirculatory phenomenon. By creating the window by removing the uncinate may be adequate. If enlargement is required, only the posterior fontanelle should be removed. The anterior fontanelle is rarely more than 1 to 2 mm in length and when undisturbed, protects the lacrimal duct. The posterior fontanelle is up to 20 mm and often encompasses the accessory ostia of the maxillary sinus. When making the posterior cut from the natural ostia, make it close to the roof of the sinus and incorporate any accessory ostia. Sharply remove the large lower flap to create the maxillary antrostomy. With the 0 degree scope the bulla is identified and its lower medial portion is removed creating a functional opening that includes its natural ostia. If there is continued mucosal abnormalities more comprehensive surgery is preformed on the anterior and posterior ethmoid cells using the Messerklinger technique. This limited surgery usually is adequate to treat most children with recalcitrant sinusitis. Revisions may be undertaken with all important landmarks intact.
The sphenoid sinus needs to be entered for a variety of conditions such as infection, mucopyoceles, mycetomas, or suspect neoplasms.
The approach to the sphenoid sinus is very precarious despite improved vision with the endoscopes. The vital anatomic structures behind the anterior sphenoid wall is variable. The internal carotid artery may be located immediately behind the wall when dehiscent, or be covered only by thin bone. The optic nerve is minimally protected. Also to be remembered are the pituitary gland and the trigeminal nerve which are rarely injured but in close proximity. The identification of the anterior wall of the sphenoid is essential.
This can be verified by two methods. First, on the medial side of the superior turbinate, the natural ostium of the sphenoid sinus is visualized. A measurement from the natural ostium to the anterior nasal spine is obtained. This measurement is then used in the surgical field lateral to the superior turbinate to the suspect posterior ethmoid wall. When the posterior ethmoid cells exists that superiorly overrides the sphenoid sinus (Onodi cells), the second measurement would be greater than the measurement to the natural ostium. The safest entry to the sphenoid is inferiomedially. Using careful dissection the wall is cleansed of all bony and mucosal septations. A rigid instrument, such as a straight suction, is placed in the inferiormedial quadrant. It is advanced as far posterior and inferiomedially then swept medially towards the septum fracturing the superior turbinate. This will expose a very consistent near-vertical fracture line which the authors (parson et al) call the 'ridge'.
Medially to this is the ethmoid fontanelle or the mucosa lateral to the superior turbinate. This will expose the natural ostia. Enlargement of the natural ostia is done using a curette taking down the lateral 'ridge' in a posterior to anterior direction. This approach is functional enlarging the natural ostium. This anterior anatomy is very consistent from young toddlers to senior citizens. In the pediatric patient, there are no standard measurements for size of the ethmoid cavity or distance relationships with regards to the sphenoid sinus. The dissection must be meticulous with strict attention to anatomic landmarks. Upon completion of the surgery packing is usually avoided and stents for the septum will be removed at the time of the first post operative cleaning. Post
Operative Management:
Postoperative medications consist of oral antibiotics, topical nasal decongestant, a topical nasal steroid, and saline nasal spray. Pediatric FESS is a staged procedure with the second stage in 2 weeks for operative cleaning. This waiting period allows sufficient healing of the surgical site but is not long enough for excessive synechia formation.
Complications:
Major complications of endoscopic sinus surgery are classified into two broad categories: orbital and intracranial. Significant complications are usually the result of poor appreciation of anatomic relationships, poor visualization, or excessive bleeding. The use of FESS in pediatric sinusitis has generated few reports of complications. Minor complications were reported in 10 % of the patients such as postoperative bleeding, ecchymosis, otalgia, dacrocystorhinitis. Adhesions were the major postoperative finding which can lead to recurrent disease. In the pediatric population, the lack of reported CSF fistulas may be secondary to less extensive surgery, less developed sinuses ( with thicker bone), or thicker dura.
Summary:
Pediatric Functional Endoscopic Sinus surgery is very controversial. There are proponents for solely medical management and then the proponent for limited endoscopic surgery. I believe that no one would take the liberal approach to this surgery as ethical or medically sound. Five to 15% of the pediatric population has had sinusitis. This may even be underestimating the incidence, but nearly all of these infections will clear with or without medication. Only the patient that has had maximal documented medical therapy or complications of sinusitis should be a candidate. One thing that may change this approach is the increasing incidence of drug resistance patterns. The multi-drug resistant pneumococci are increasing at a staggering rate. This is also starting to show up with H. influenza becoming less sensitive to antibiotics, with a noticeable upward creep in MIC's to beta-lactam and frank resistance to sulfa. M. catarrhalis is resistant to beta-lactam and clinical failures have been seen with the new generation cephalosporins. The net result is that chasing pediatric sinusitis with oral antibiotics is becoming increasingly difficult. The treatment should be based on cultures and sensitivities rather than empiric therapy.
Many recent articles have reviewed their results on pediatric sinus surgery which has been very favorable with few complications. Lazar et al out of 210 patients had a 79% relief of symptoms. 80% of asthmatic reported improvements in asthma after FESS. Failures were seen in patients who had refractory disease or had other systemic problems such as immunodeficiency, Cystic fibrosis or immotile cilia syndrome. Parsons et showed a greater than 80% improvement after FESS with his series of 550 patients. There is a definite role for pediatric endoscopic sinus surgery.
DISCUSSION
Comments on Grand Rounds of Jan. 18, 1995
On Pediatric Sinusitis and Surgical Treatment
By Ronald W. Deskin, M.D., UTMB Department of Otolaryngology
Healthy paranasal sinuses in children depend on good ventilation and drainage, good mucociliary clearance and normal systemic immunity. In children the development and maturation of these systems is a specific developmental process and sinusitis tends to be age related showing marked improvement in most cases by age seven to eight years.
In previous years little emphasis and importance was placed on the entity of pediatric sinusitis. In many areas this pendulum has now swung back to the point that surgical solutions are almost demanded for the problem of chronic rhinorrhea in children. The promotion of newer surgical techniques, some of which are unproven in the small child, new sinus imaging techniques, and the growing problem of working couples with children in day care who face a dilemma in keeping their children well enough to stay in day care so that the parents may work have all contributed to the attitude. The growing concern that sinus infections can effect the health of children with chronic pulmonary disease has also brought sinusitis and its treatment to the foreground.
It is very difficult to define chronic sinusitis in children and how much recurrent sinusitis is too much. The work up, if conditions are appropriate, should include allergic evaluation, immune globulin evaluation and in some cases respiratory ciliary biopsy. Plain x-rays are of limited value and CT scans should not be ordered unless surgery is anticipated because of acute suppurative complications, evaluation of the child with chronic pulmonary disease who flares up with each episode of acute sinusitis, and in those children who have failed to respond to adequate medical management and who are felt to have true chronic disease affecting overall health and quality of life. This last indication is very difficult to define in children. Adenoidectomy and sinus irrigation may be helpful for improvement in the child under five to six years of age with recurrent purulent rhinorrhea and nasal obstruction symptoms.
After maximum medical management has been attempted and failed, surgical indications may be present. Endoscopic sinus surgery allows better visualization, eliminates the need for facial incisions and promotes physiologic drainage. Minimal endoscopic sinus surgery such as partial uncinate removal and opening of the ethmoid bulla may be adequate for most children who are candidates for endoscopic sinus surgery.
Complications of Endoscopic Sinus Surgery...prevention and management.
The history of nasal endoscopy and of endoscopic sinus surgery parallels advances made in the development of instruments suitable for examining the small confines of the nose, nasopharynx and the paranasal sinuses. Bozzini is credited for the development and use of the first "light conductor.".
Subsequently, Czermak, who coined the term "rhinoscopy," popularized the use of the nasal speculum, an instrument that unknownst to him had already been in use during the first century in Pompeii. In 1879, the Nitze-Leiter cystoscope with a platinum wire light source, was modified into the first endoscope bearing any resemblance to today's modern scopes, the Storz Fiberoptic Endoscope, which was developed in the mid-1950's. These advances, along with the development of computed tomography, made it possible for clinicians to localize sinus disease and thereby redirect their therapeutic interventions.
Messerklinger is credited as the first to develop a systematic approach to diagnosing and treating sinus inflammatory disease. He noted that despite the seemingly extensive nature of the disease process in remote areas of the nose and paranasal sinuses, in most cases these observations could be explained by relating anatomical form to function. The frontal, maxillary and anterior ethmoid sinuses converge on a rather limited area known as the ethmoid infundibulum, which comprises one component of the osteomeatal unit. Other structures in this area include the uncinate process, the middle turbinate and the ethmoid bulla. Physiologically, this area is important in the etiology of inflammatory sinus disease.
Obstruction either by inflammation, polyp, tumor, or by dysfunction of the normal mucociliary clearance mechanisms in this area leads to primary disease that can progress and cause contiguous infection of the larger paranasal sinuses, or secondary disease.
Functional endoscopic sinus surgery is based on the premise that removing the obstruction to normal mucociliary clearance in the area of the OMC will lead to subsequent clearance of secondary disease and restoration of normal mucociliary clearance. This is in contrast to more extensive interventions in which nearly all accessible mucosa is debrided. Although this is sometimes necessary, as in severe nasal polyposis, such extensive procedures usually are not required and add to the overall risk of complications.
Early in this century, Mosher stated that intranasal ethmoidectomy is "the blindest and most dangerous operation in all of surgery." While this may have been true then, the endoscopic approach to intranasal surgery has afforded surgeons unparalleled illumination and clarity of the surgical field. Despite these advances, with their attendant reductions in morbidity and mortality, complications remain a real concern when performing ESS. They are divided into major complications including: death, intracranial hematoma, massive hemorrhage, blindness, orbital hematoma, and CSF leak, and minor complications including synechiae, orbital emphysema, acute asthma exacerbation, epiphora, hyposmia, anosmia and dysgeusia.
In the first U.S. study that quantified complications related to ESS, Stankiewicz, reported a 6% major and 13% minor complication rate, the most common being synechiae. In a follow-up study, Stankiewicz reported on the complication rate of a subsequent group of 90 patients, and noted a rate of 2.4%, which compared favorably with previous reports of complications as reported by Freedman and Kern in 1979 using conventional intranasal methods. This significant drop in the complication rate was attributed to greater operative experience, concurrent cadaveric dissection, and the use of limited ethmoidectomy initially, with gradual progression to more extensive procedures.
Several studies have subsequently demonstrated a further decline in the incidence of complications. Dessi noted a 1.2% complication rate for overall complications.
There are several general aspects that impact on the risk of performing ESS. First is patient selection. Multiple studies have cited an increased risk of complications associated with ESS performed on patients with polyposis, prior surgical intervention and in those who have had long-standing disease. Dessi noted that all 5 of his complications occurred in patients being operated on for significant polyposis.
The type of anesthesia utilized has been debated. Those espousing local techniques cite the patient's ability to convey painful stimuli when the skull base or peri-orbita is encroached upon as well as a significantly lower blood loss. However, this requires both a compliant patient and an optimal topicalization of the nose by the surgeon. Alternatively, other authors recommend general anesthesia in addition to topical preparation of the nose citing greater patient comfort, especially in more extensive procedures. Stankiewicz (1989) reported in a series of 180 patients that there was no difference in the rate of complications when either technique was used. He did note, however, that blood loss was greater in those procedures done under general anesthesia.
Meticulous hemostasis and atraumatic technique are essential. Several authors have emphasized the need to ensure adequate visualization. If bleeding precludes an adequate view, the procedure should be stopped until hemostasis is achieved or terminated if this is not possible.
Functional ESS, which espouses a more limited approach, can and should be used whenever the disease process dictates its appropriateness. Smith and Brindley, utilizing this approach, found comparable results when compared with studies using more extensive interventions. Experience of the surgeon, as alluded to earlier, plays a large part in determining the risk of an adverse outcome.
Finally, familiarity with endoscopic anatomy and its variations play an extremely important part in reducing complications. As in all of surgery, anatomical landmarks are critical to maintaining spatial orientation. This is also true in the nasal cavity. The close proximity of the ethmoid sinuses to the skull base and brain as well as the orbit and optic nerve mandates continuous awareness of one's location. Streitmann et al studied 50 cadaveric heads and performed several measurements from the base of the columella to various important landmarks, relating both the angle of incidence and the distance to these structures.
Ohnishi identified 5 high-risk areas that he considered to merit special attention during ESS. The lamina papyracea, given its protrusion into the field and its relative fragility, is an area that is frequently violated. Injury in this area predisposes to medial rectus entrapment or transection. Extensive manipulation in this region has resulted in blindness in some cases. The anterior ethmoid artery and roof are likewise in a susceptible location, and injury laterally can predispose to either significant hemorrhage into the field or to orbital hematoma if the vessel retracts in its bony canal. Injury more medially, with fracture of the attenuated ethmoid roof, is a common cause for CSF leak and predisposes to possible meningitis. The lateral lamella of the cribriform plate (also the lateral wall of the olfactory bulb) is an area where attempts at complete exenteration of superior ethmoid air cells can result in small dehiscences that predispose to increased risk of infection. The posterior ethmoid roof and artery, although usually not problematic, may present with a dehiscent artery lying inferior to the roof, with or without a bony canal. Finally, the area Between the posterior ethmoid and the sphenoid sinus is of critical significance because it is here where anatomical variations can predispose to inadvertent injury to the optic nerve or the carotid artery. Takedown of thick bony buttresses in this area should not be performed as fracture planes can be created that run into the carotid artery bony canal with possible pseudoaneurysm formation or fistulization to the cavernous sinus.
As important as familiarity with normal anatomy is, it is of equal importance to be aware of the anatomical variants that one might encounter in performing ESS. Bolger, in a detailed analysis of 202 consecutively-imaged patients, identified several bony anatomic variations. The most common of these, the agger nasi, which was present in 98.5% of patients, is described as being the most anterior of the anterior ethmoid cells, bounded superiorly by the frontal sinus. These can be quite large, may displace the lamina papyracea to a more lateral position. A concha bullosa (or pneumatized middle turbinate) was present in 53% of cases. No consistent relationship between the presence of this variation and the pathogenesis of OMC disease has been established. The need for resection of these should proceed on a patient-to-patient basis, as these may be the reason for primary disease at the OMC.
Haller's Cells are ethmoid cells that project into the maxillary sinus. Although it was present in 45% of scans, not all Haller cells are pathologically important. Again, case-by-case evaluation of these entities is required to assess their role in contributing to maxillary ostium blockage.
The Onodi Cell is a posterior ethmoid cell that has encroached upon the area of the sphenoid sinus. It is of considerable significance because in a large majority of these, a frankly dehiscent optic nerve, carotid artery or both may be present in variable locations. Several other variants have been described.
Among these are the uncinate bulla, which although relatively infrequent, may alter the anatomy at the OMC. Others include Bulla Gali (5.4%), pterygoid pneumatization (43.6%), and anterior clinoid pneumatization (13.3%). Preoperative recognition of these variations is useful as these at times may require special attention in order to prevent postoperative recurrent disease, and more importantly, complications by allowing the surgeon to better estimate the limits of resection.
I would now like to discuss the prevention and management three complications, that, if detected early, can be dealt with before more severe delayed sequelae evolve. These include massive hemorrhage, cerebrospinal fluid leak, and orbital hematoma. The management of synechiae and of nasolacrimal duct obstruction will also be briefly reviewed.
Massive hemorrhage, resulting from major vascular injury, is an exceedingly rare complication. Avoidance of complications in this area requires familiarity with the variations that occur with respect to the ICA. The lateral sphenoid wall usually demonstrates an inward bulge harboring the ICA occasionally associated with the optic nerve lying superior to it. Kennedy et al noted that in 22% of 188 sphenoid sinuses examined, there was dehiscence of the bony canal over the ICA. In three cases, the artery was found to be completely dehiscent in the posterior wall of the posteriormost ethmoids. Near-midline ICA's were seen in one case. It is believed that these anomalies account for the reported cases of ICA injury. These reports led to the development of the carotid drill by Sofferman.
In the event of carotid artery injury with massive hemorrhage, nasal packing should be placed immediately with manual compression of the ipsilateral cervical ICA. Controlled hypotension, blood products and neurosurgical and neuroradiological consultation should be called. Carotid angiography should then be undertaken. If this should indicate a significant carotid injury, balloon occlusion is attempted with EEG surveillance. If no changes occur on EEG, then carotid artery ligation may be performed. If there is evidence of lateralization on EEG with occlusion, then the balloon should be deflated and the packing left in place. In the ICU, Swan-Ganz catheterization and hypervolemic therapy should be implemented to optimize cerebral perfusion. Once this has been attained, occlusion should be reattempted. If evidence of adequate collateralization is present, then the carotid may be ligated. If not, then the patient should continue to be observed, and an attempt at removal of packing in the operating room should be attempted at a later time.
CSF leak resulting from penetration of the skull base near the area of the ethmoids or the sphenoids occurs in approximately 1% of cases. Preservation of the middle turbinate as a landmark is of critical importance in preventing complications. One should always operate lateral to its origin, since medial dissection can violate the thinner and lower cribriform plate. Although thicker than the cribriform, the fovea ethmoidalis is still susceptible to fracturing, especially medially. Therefore, one should try to remain as close to the lamina papyracea as possible when approaching the frontal recess. Similarly, the middle turbinate is important in locating the sphenoid sinus posteriorly, as its anterior wall lies in a plane between the superior inferior turbinate and the lower aspect of the middle turbinate. On average, the sphenoid sinus lies 7 centimeters posterior to the nasal introitus. This wall is very thin and should not require excessive force to infracture. Undue resistance implies that basilar skull bone is being impinged upon and that landmarks need to be reidentified.
CSF leaks noted intra-operatively can be repaired primarily using either temporalis fascia, septal or turbinate mucosa or fascia lata. The graft is placed over the defect and tucked under the bony edges as seen here. Muscle is then placed over this followed by Gelfoam for support. Leaks of the sphenoid sinus have been managed by plugging the defect with fibrin glue and Gelfoam followed by Gelfoam obliteration of the sphenoidotomy. Delayed fistula can be managed with bedrest with or without a lumbar drain. If this fails to resolve within 2 to 3 weeks, exploration either endoscopically with flourescein, extranasally or intranasally, or via craniotomy may be necessary. The use of antibiotics as prophylaxis against CNS infection is controversial.
Orbital complications, including blindness and diplopia, occur via two mechanisms: direct injury to the optic nerve or extraocular muscles, which is rare; and retro-orbital hematoma. Injury to either the anterior or posterior ethmoidal arteries or penetration of the lamina papyracea can lead to trace edema, periorbital and lid ecchymosis, chemosis and minimal proptosis, and may progress to massive proptosis with temporary loss of vision. If this is not rapidly addressed by the surgeon, persistent elevation of intraocular pressure with compromise of venous outflow leads to retinal ischemia with resultant permanent blindness. Use of general anesthesia increases risk as the patient is no longer able to sense pain when the lamina or ethmoid roof is injured. The eyes should remain uncovered and checked routinely by the surgeon in order to assess proptosis early. One should remember that the lamina papyracea lies superior and lateral to the natural maxillary ostium. Of note, several studies have cited a significantly greater incidence of orbital complications on the left side. This reflects an alteration in how the right-handed surgeon perceives the location of the ethmoids. On the right, they lie directly posterior as one would expect. On the left, however, scope orientation alters the view giving the surgeon the impression that the lamina papyracea is more lateral when in actuality it is more medial. Gentle palpation of the eye while dissecting in the area allows one to identify the lamina prior to entering it. Exposure of orbital fat in and of itself is usually of no consequence. However, a careful inspection of the eye should be undertaken. If signs of orbital hematoma are present, the patient should be admitted and observed as delayed blindness up to 48 hours post-op have been documented. Orbital packs should be avoided as these may increase intraorbital pressure. Management of an intraoperative orbital hematoma entails immediate ophthalmologic consultation and institution of several methods aimed at reducing intraorbital pressure. Eye massage is effective in that it helps to redistribute intraocular and extraocular fluids. This maneuver is absolutely contraindicated in patients with a prior history of ophthalmic surgery including corneal, retinal, or glaucoma filtering surgery. Acetazolamide 500 mg. IV can reduce intraorbital pressure by decreasing aqueous humor production, however its onset of action is slow. Mannitol has a much quicker onset and acts by osmotically drawing fluid out of the orbital spaces. A dose of 1-2 GRAMS per kilogram given over 20-30 minutes is usually safe and effective. Miotics should be avoided as these interfere with pupillary responses and thereby confuse the clinical picture. The use of steroids for this condition is not clear. Currently, no studies have shown a therapeutic gain associated with their use. Should medical management fail, lateral canthotomy has proven effective in reducing intraorbital hypertension. Briefly, the technique entails releasing the lateral canthal structures, including the lateral canthal tendon, by placing a straight hemostat across the area followed by sharp division of these structures down to the periorbital fascia. If this is not effective, medial canthotomy via the Lynch external ethmoidectomy approach can be performed with satisfactory results. Postoperative monitoring with diuretics in consultation with ophthalmology is usually uneventful.
Nasolacrimal duct stenosis resulting from middle meatal antrostomy is uncommon. It is presumed that the nasolacrimal duct is injured more frequently, but few cases result in frank obstruction with epiphora. Regardless, a few points are worthy of mention. First, it should be remembered that the nasolacrimal duct lies only 3-6 millimeters anterior to the natural ostium of the maxillary sinus and that the antrostomy should be made no further forward than the anterior end of the middle turbinate. If hard bone is encountered anteriorly, this likely represents a natural bony septum separating the ostium from the canal, or the lacrimal duct canal itself and should not be violated. Cases of persistent epiphora can be managed with serial lacrimal probing. Formal dacryocystorhinostomy, either endoscopically or via the external approach or both can be performed if necessary. A combined approach is currently favored in which the lacrimal sac is cannulated with a light source and endoscopically, the area of the lacrimal sac is identified, stripped of its bony and mucosal covering, and marsupialized into the frontal recess.
Finally, synechiae usually results from fibrous scar band formation between the lateral nasal wall and the middle and/or inferior turbinates. Atraumatic technique and stenting in these areas have been shown to be useful, but invariably, reduced incidence of this outcome results from meticulous debridement postoperatively in the office. Partial middle turbinectomy has been implemented by several authors with mixed results.
Major complications in endoscopic sinus surgery are rare. However, when they do occur they can be catastrophic and it behooves the surgeon to identify these problems early before permanent deficits evolve. Practical knowledge of the anatomy, both normal and variant, is requisite. Prevention of complications based on technique and implementation of limited surgery based on extent of disease are well established. Management strategies aimed at minimizing or reversing adverse events exist and these should be familiar to the endoscopic sinus surgeon.

Case Presentation
A 54-year-old female with a long-standing history of chronic sinusitis and nasal polyposis presented with symptoms of bilateral frontal, retro-orbital, and midfacial pain, nasal obstruction, purulent post-nasal drip and halitosis. Her past medical history was significant for hypertension and arthritis. Her medications included Beconase, Seldane, Augmentin, Capoten and Premarin. She denied allergy to aspirin. On exam, she was noted to have minimal maxillary and frontal sinus tenderness. Anterior rhinoscopy showed streaking of purulent material across the middle turbinates bilaterally, large inferior turbinates, leftward septal deviation and polyps of the left osteomeatal complex. All extraocular muscle movements were intact. The remainder of her physical exam was unremarkable.
A CT scan of the nose and paranasal sinuses without contrast revealed complete opacification of the right maxillary, ethmoid, frontal and sphenoid sinuses. The left maxillary, ethmoid, frontal, and sphenoid sinuses were opacified to varying degrees. Paradoxical curvature of the right inferior turbinate was also noted.
The patient underwent endoscopic sinus surgery consisting of bilateral anterior and posterior ethmoidectomy, middle meatal antrostomy, and sphenoidotomy. Four months post-operatively, she demonstrated signs and symptoms of epiphora of the left eye. Despite conservative therapy, her symptoms persisted.
She subsequently underwent septoplasty and partial resection of her inferior turbinate for persistent nasal obstruction, at which time a dacryocystorhinostomy was performed on the left side. Six months post-operatively, she is doing well, remains asymptomatic with regard to her sinus symptoms, and has not experienced any repeat episodes of epiphora.
Orbital Complications of Endoscopic Sinus Surgery Endoscopic sinus surgery is considered by many to be the most exciting development in otolaryngology. The aim is to restore the natural mucociliary clearance mechanism, drainage, and aeration of the sinuses by a minimally invasive technique, maintaining as much of the normal anatomy as possible.2 We agree with the authors that the incidence of ocular complications is low and similar to those reported by other non-endoscopic approaches.3 The authors mentioned CT scanning as a preoperative measure to reduce complications; this is a well established practice in all departments that practise endoscopic sinus surgery. Orbital complications are more likely to occur in patients with extensive polyposis especially those who had multiple surgery; however, in a survey of British otolaryngologists4 the overall estimated complication rate was 0.24%. As a matter of fact endoscopic sinus surgery techniques are being used to treat orbital complications such as malignant exophthalmos in thyroid eye disease.5 We believe that the key to avoiding such complications is the adequate understanding of the nasal anatomy endoscopically, which is only achieved through attending specialised workshops that are widely available throughout the country; adequate haemostasis intraoperatively is of paramount importance. If complications are encountered then the immediate termination of the procedure is recommended and an urgent ophthalmological opinion should be sought |



 The computed tomographic (CT) scan illustrates the proximity of the ethmoid sinus to the other sinuses and adjacent important structures. This scan also shows a defect (white arrow) in the roof of the right ethmoid sinus, from which cerebral spinal fluid is draining into the nose.
The computed tomographic (CT) scan illustrates the proximity of the ethmoid sinus to the other sinuses and adjacent important structures. This scan also shows a defect (white arrow) in the roof of the right ethmoid sinus, from which cerebral spinal fluid is draining into the nose.  Original illustration of Nathanial Highmore showing the maxillary sinus, c. 1651 (courtesy of the New York Academy of Medicine Library).
Original illustration of Nathanial Highmore showing the maxillary sinus, c. 1651 (courtesy of the New York Academy of Medicine Library).  Endoscopic image showing identification of the uncinate process (up) and probing of the space immediately behind it, the ethmoid infundibulum, by a hook-like instrument known as an ostial seeker. The middle turbinate (mt) is an appendage of the ethmoid sinus and an important surgical landmark..
Endoscopic image showing identification of the uncinate process (up) and probing of the space immediately behind it, the ethmoid infundibulum, by a hook-like instrument known as an ostial seeker. The middle turbinate (mt) is an appendage of the ethmoid sinus and an important surgical landmark..  Removal of the uncinate process with a surgical debrider reveals the ostium of the maxillary sinus. This form of antrostomy permits inspection of the maxillary sinus and removal of polyps or other abnormal findings from within the sinus.
Removal of the uncinate process with a surgical debrider reveals the ostium of the maxillary sinus. This form of antrostomy permits inspection of the maxillary sinus and removal of polyps or other abnormal findings from within the sinus.  A surgical curette is shown removing the cells of the posterior ethmoid sinus. The boundaries of the ethmoid sinus are the lamina papyracea (lp), the middle turbinate (mt) and the floor of the anterior cranial fossa or skull base. The lamina papyracea or orbital plate is a thin vertical plate of bone which separates the ethmoid sinus from the orbit. In sinus surgery, each of these boundaries should be visualized and with the possible exception of the middle turbinate, preserved intact.
A surgical curette is shown removing the cells of the posterior ethmoid sinus. The boundaries of the ethmoid sinus are the lamina papyracea (lp), the middle turbinate (mt) and the floor of the anterior cranial fossa or skull base. The lamina papyracea or orbital plate is a thin vertical plate of bone which separates the ethmoid sinus from the orbit. In sinus surgery, each of these boundaries should be visualized and with the possible exception of the middle turbinate, preserved intact.  Sagittal, or midline cadaver section through the ethmoid sinus. On the right is the sphenoid sinus (SS) and on the left is the external nose. The area through which the frontal sinus drains into the nose is known as the frontal recess (FR). This section illustrates the removal the inferior or lower ethmoid cells which are encompassed by the dotted line as the procedure progresses from the front to back of the nose.
Sagittal, or midline cadaver section through the ethmoid sinus. On the right is the sphenoid sinus (SS) and on the left is the external nose. The area through which the frontal sinus drains into the nose is known as the frontal recess (FR). This section illustrates the removal the inferior or lower ethmoid cells which are encompassed by the dotted line as the procedure progresses from the front to back of the nose.  The same cadaver section illustrates the back to front (see arrow) removal of the upper ethmoid cells which are outlined by a dotted line.
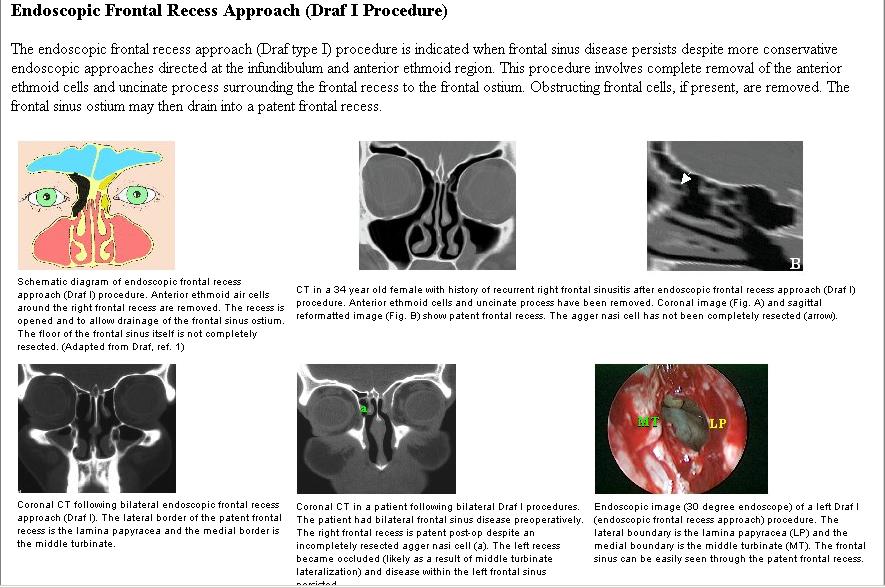
The same cadaver section illustrates the back to front (see arrow) removal of the upper ethmoid cells which are outlined by a dotted line.  Illustration of frontal sinusitis (1, orange) secondary to obstruction of the frontal recess (2, yellow). Such obstruction could be secondary to nasal polyps, scarring from prior surgery or variations in anatomy of the frontal recess (such as the uncinate process or ethmoid cells obstructing frontal sinus drainage).
Illustration of frontal sinusitis (1, orange) secondary to obstruction of the frontal recess (2, yellow). Such obstruction could be secondary to nasal polyps, scarring from prior surgery or variations in anatomy of the frontal recess (such as the uncinate process or ethmoid cells obstructing frontal sinus drainage).  Type I endoscopic frontal sinusotomy. Intraoperative photograph shows the frontal sinus (FS) is exposed after removal of anterior ethmoid cells. As the diseased mucous membrane and remaining anterior ethmoid cells were removed, the entire frontal sinus became evident (dotted line).
Type I endoscopic frontal sinusotomy. Intraoperative photograph shows the frontal sinus (FS) is exposed after removal of anterior ethmoid cells. As the diseased mucous membrane and remaining anterior ethmoid cells were removed, the entire frontal sinus became evident (dotted line).  Illustration of type II frontal sinusotomies. Type IIa consists of removing the floor of the frontal sinus between the lamina papyracea (the bony wall separating the orbit from the ethmoid sinus) and the middle turbinate. Type IIb frontal sinusotomy in the removal of the entire floor of the frontal sinus. Unlike a type III frontal sinusotomy, the nasal septum and intra-frontal septum are undisturbed.
Illustration of type II frontal sinusotomies. Type IIa consists of removing the floor of the frontal sinus between the lamina papyracea (the bony wall separating the orbit from the ethmoid sinus) and the middle turbinate. Type IIb frontal sinusotomy in the removal of the entire floor of the frontal sinus. Unlike a type III frontal sinusotomy, the nasal septum and intra-frontal septum are undisturbed.  Coronal CT scan of patient with bilateral frontal sinusitis (1) secondary to extension of ethmoid cells (2, also described previously as a frontal cell) into the floor of the frontal sinus. These ethmoid cells literally balloon into the floor of the frontal sinus and are visible due to the contrast between the mucous in the frontal and ethmoid sinuses (1) and the air within the ethmoid or frontal cells (3).
Coronal CT scan of patient with bilateral frontal sinusitis (1) secondary to extension of ethmoid cells (2, also described previously as a frontal cell) into the floor of the frontal sinus. These ethmoid cells literally balloon into the floor of the frontal sinus and are visible due to the contrast between the mucous in the frontal and ethmoid sinuses (1) and the air within the ethmoid or frontal cells (3).  A. Ethmoid cell or frontal cell (green ellipse) extending into the floor of the frontal sinus.
A. Ethmoid cell or frontal cell (green ellipse) extending into the floor of the frontal sinus.  B. Restoring drainage of the frontal due to an obstructing frontal cell has been likened to removing an egg from an inverted egg cup (dotted blue line [Stammberger, 2000]).
B. Restoring drainage of the frontal due to an obstructing frontal cell has been likened to removing an egg from an inverted egg cup (dotted blue line [Stammberger, 2000]).  Intraoperative photograph demonstrates the Stammberger analogy of removing an egg from an inverted egg cup as visualized from the perspective of being within the cup (Stammberger, 2000). The top of the inside of the egg is the upper surface of the frontal cell (1). The egg cup is the surrounding bony perimeter of the frontal recess and frontal sinus. The forceps (2) are shown beginning the removal of the egg (i.e., the frontal cell) without injuring the egg cup.
Intraoperative photograph demonstrates the Stammberger analogy of removing an egg from an inverted egg cup as visualized from the perspective of being within the cup (Stammberger, 2000). The top of the inside of the egg is the upper surface of the frontal cell (1). The egg cup is the surrounding bony perimeter of the frontal recess and frontal sinus. The forceps (2) are shown beginning the removal of the egg (i.e., the frontal cell) without injuring the egg cup.  As the ethmoid cell (EC) is removed the frontal sinus (FS) becomes visible.
As the ethmoid cell (EC) is removed the frontal sinus (FS) becomes visible.  Further removal of the ethmoid cell reveals part of the frontal sinus. As surgery further progressed, the remaining ethmoid cell was removed (encompassed by green dotted line) leaving the mucous membrane lining the frontal recess (blue dotted line) intact.
Further removal of the ethmoid cell reveals part of the frontal sinus. As surgery further progressed, the remaining ethmoid cell was removed (encompassed by green dotted line) leaving the mucous membrane lining the frontal recess (blue dotted line) intact.  The elements of type III frontal sinusotomy are removal of the entire floor of both frontal sinuses, the intrasinus septum which divides the frontal sinus into a left and right cavity and upper nasal septum.
The elements of type III frontal sinusotomy are removal of the entire floor of both frontal sinuses, the intrasinus septum which divides the frontal sinus into a left and right cavity and upper nasal septum.  Intraoperative CT reconstruction utilizing computer assisted image guided surgery. In this image, the end of a probe placed within the right frontal is identified as the convergence of the vertical and horizontal lines. To restore drainage of the frontal sinus, the floor of the sinus (1) is removed as are the intrasinus septum (2) and the upper nasal septum (3).
Intraoperative CT reconstruction utilizing computer assisted image guided surgery. In this image, the end of a probe placed within the right frontal is identified as the convergence of the vertical and horizontal lines. To restore drainage of the frontal sinus, the floor of the sinus (1) is removed as are the intrasinus septum (2) and the upper nasal septum (3).  Illustration of sagittal (midline) section through right sphenoid sinus. This drawing emphasizes the important neurologic and vascular structures which border the outer wall of the sphenoid sinus. As infectious or neoplastic disease progresses within the sphenoid sinus, patients can develop symptoms referable to any of illustrated nerves or vessels. For example, tumors or infection encroaching upon the maxillary nerve would give rise to mid-face pain. Disease involving the optic nerve would initially present with partial loss of temporal vision (peripheral or lateral vision) and progress to total blindness (modified from Rice DH, Schaefer SD. Endoscopic Paranasal Sinus Surgery, 3rd Ed. Lippincott; Philadelphia. 2003.
Illustration of sagittal (midline) section through right sphenoid sinus. This drawing emphasizes the important neurologic and vascular structures which border the outer wall of the sphenoid sinus. As infectious or neoplastic disease progresses within the sphenoid sinus, patients can develop symptoms referable to any of illustrated nerves or vessels. For example, tumors or infection encroaching upon the maxillary nerve would give rise to mid-face pain. Disease involving the optic nerve would initially present with partial loss of temporal vision (peripheral or lateral vision) and progress to total blindness (modified from Rice DH, Schaefer SD. Endoscopic Paranasal Sinus Surgery, 3rd Ed. Lippincott; Philadelphia. 2003.  MRI of patient with acute left sphenoid sinusitis refractive to antibiotic therapy. This patient complained of intense mid face and vertex pain. As is seen in this patient, the sphenoid sinus may extend beyond the body of the sphenoid bone to pneumatize or involve the adjacent regions. In this case, a lateral recess has been formed within the greater wing of the sphenoid sinus. This image illustrates the close proximity of important brain, eye and blood vessels to the sphenoid sinus.
MRI of patient with acute left sphenoid sinusitis refractive to antibiotic therapy. This patient complained of intense mid face and vertex pain. As is seen in this patient, the sphenoid sinus may extend beyond the body of the sphenoid bone to pneumatize or involve the adjacent regions. In this case, a lateral recess has been formed within the greater wing of the sphenoid sinus. This image illustrates the close proximity of important brain, eye and blood vessels to the sphenoid sinus.  Saggital cadaver section shows exposure of the anterior wall of the sphenoid sinus (SS) by performing a total ethmoidectomy. Alternately, the posterior-inferior half of the middle turbinate can be removed to expose the sinus and the sphenoid ostium (SO, white circle).
Saggital cadaver section shows exposure of the anterior wall of the sphenoid sinus (SS) by performing a total ethmoidectomy. Alternately, the posterior-inferior half of the middle turbinate can be removed to expose the sinus and the sphenoid ostium (SO, white circle).  Endoscopic photograph showing the approximate location of the sphenoid sinus ostium (opening of the sphenoid sinus into the nose) relative to the middle turbinate (mt) and the lateral nasal wall. One more anterior lateral nasal wall structures is the uncinate process (up), which is the most anterior element of the osteomeatal complex (or middle meatus) or primary drainage site of the ethmoid, maxillary and frontal sinuses. The sphenoid sinus drains independently of the middle meatus, and medial to the posterior insertion of the middle turbinate.
Endoscopic photograph showing the approximate location of the sphenoid sinus ostium (opening of the sphenoid sinus into the nose) relative to the middle turbinate (mt) and the lateral nasal wall. One more anterior lateral nasal wall structures is the uncinate process (up), which is the most anterior element of the osteomeatal complex (or middle meatus) or primary drainage site of the ethmoid, maxillary and frontal sinuses. The sphenoid sinus drains independently of the middle meatus, and medial to the posterior insertion of the middle turbinate.  Saggital cadaver section illustrating the relationship of the sphenoid sinus (SS) ostium (black arrow) to the middle turbinate (mt), the posterior tip of the middle turbinate (white arrow), ethmoid sinus (ES) and pituitary gland (pg).
Saggital cadaver section illustrating the relationship of the sphenoid sinus (SS) ostium (black arrow) to the middle turbinate (mt), the posterior tip of the middle turbinate (white arrow), ethmoid sinus (ES) and pituitary gland (pg).  As reported by Harris Mosher, the average distance of the sphenoid sinus ostium is 7 cm from the anterior nasal spine to the face of the sinus at an angle of 30 degrees from the floor of the nose (Mosher, 1929). As this measurement is frequently cited, it is important to remember that Mosher was reporting an average and that there is significant variation between patients.
As reported by Harris Mosher, the average distance of the sphenoid sinus ostium is 7 cm from the anterior nasal spine to the face of the sinus at an angle of 30 degrees from the floor of the nose (Mosher, 1929). As this measurement is frequently cited, it is important to remember that Mosher was reporting an average and that there is significant variation between patients.  Approximate removal of anterior wall of sphenoid sinus is illustrated (white arrow, outlined in white).
Approximate removal of anterior wall of sphenoid sinus is illustrated (white arrow, outlined in white).  Axial CT scan of a patient with thyroid eye disease. Several of the elements of this disease are evident on this image: 1) exophthalmos or protrusion of the eye ball from the orbit, and 2) enlargement of the extraocular muscles, including the medial rectus (mr). Also seen are some less common variations of sinus anatomy. Specifically, a posterior ethmoid cell (EC) has extended into the sphenoid bone to pneumatize the area around the optic nerve.
Axial CT scan of a patient with thyroid eye disease. Several of the elements of this disease are evident on this image: 1) exophthalmos or protrusion of the eye ball from the orbit, and 2) enlargement of the extraocular muscles, including the medial rectus (mr). Also seen are some less common variations of sinus anatomy. Specifically, a posterior ethmoid cell (EC) has extended into the sphenoid bone to pneumatize the area around the optic nerve.  Coronal cadaver section illustrating the four types of orbital decompression. These are: (1) removal of the superior wall (Naffziger), (2) medial wall removal (Sewell), (3) lateral wall removal (Krönlein), and (4) removal of the floor of the orbit.
Coronal cadaver section illustrating the four types of orbital decompression. These are: (1) removal of the superior wall (Naffziger), (2) medial wall removal (Sewell), (3) lateral wall removal (Krönlein), and (4) removal of the floor of the orbit.  Intra-operative photo showing removal of the lamina papyracea during medial wall decompression of the left eye for Graves’ disease. This patient has also undergone the removal of the anterior wall of the sphenoid sinus (SS) or sphenoidotomy to expose the orbital apex.
Intra-operative photo showing removal of the lamina papyracea during medial wall decompression of the left eye for Graves’ disease. This patient has also undergone the removal of the anterior wall of the sphenoid sinus (SS) or sphenoidotomy to expose the orbital apex.  As this patient is also undergoing removal of the medial wall of the left optic canal, bone removal is continued into the sphenoid sinus (SS).
As this patient is also undergoing removal of the medial wall of the left optic canal, bone removal is continued into the sphenoid sinus (SS).  to permit herniation of orbital fat into the ethmoid sinus") After completion of all bone removal, the periorbita is incised (arrow) to permit herniation of orbital fat into the ethmoid sinus. This step should always be performed after removal of all orbital bone because the fat would otherwise reduce visualization of the remaining bone.
After completion of all bone removal, the periorbita is incised (arrow) to permit herniation of orbital fat into the ethmoid sinus. This step should always be performed after removal of all orbital bone because the fat would otherwise reduce visualization of the remaining bone.  Fat (arrow) is shown herniating through the incised periorbita into the ethmoid sinus. As the fat expands from the orbit into the sinus, the pressure or crowding of muscles and fat, is reduced.
Fat (arrow) is shown herniating through the incised periorbita into the ethmoid sinus. As the fat expands from the orbit into the sinus, the pressure or crowding of muscles and fat, is reduced.  Self-irrigating diamond burr is shown thinning the bone over the medial optic canal (arrow) in optic nerve decompression. Immediately posterior or behind this site is the internal carotid artery which is a major arterial supply to the brain. Therefore, such surgery is performed with great care.
Self-irrigating diamond burr is shown thinning the bone over the medial optic canal (arrow) in optic nerve decompression. Immediately posterior or behind this site is the internal carotid artery which is a major arterial supply to the brain. Therefore, such surgery is performed with great care.  Optic nerve decompression is complete with the removal of the remaining thinned bone over the optic nerve with micro-curette or other instruments designed for this purpose. We do not recommend removing all of the bone with a diamond burr because of potential injury to the optic nerve by the burr.
Optic nerve decompression is complete with the removal of the remaining thinned bone over the optic nerve with micro-curette or other instruments designed for this purpose. We do not recommend removing all of the bone with a diamond burr because of potential injury to the optic nerve by the burr.  Coronal cadaver section illustrating potential sites of CSF rhinorrhea. A breach in the anterior cranial fossa floor (ACF) or middle cranial fossa floor provides a route for drainage of CSF to the nose. These routes include via the posterior wall of the frontal sinus (FS), roof of the ethmoid sinus (ES), sphenoid sinus (SS), and middle cranial fossa through the roof of the middle and inner ear to the eustachian tube (ET) to the nasopharynx (the space behind the nose which communicates with the throat).
Coronal cadaver section illustrating potential sites of CSF rhinorrhea. A breach in the anterior cranial fossa floor (ACF) or middle cranial fossa floor provides a route for drainage of CSF to the nose. These routes include via the posterior wall of the frontal sinus (FS), roof of the ethmoid sinus (ES), sphenoid sinus (SS), and middle cranial fossa through the roof of the middle and inner ear to the eustachian tube (ET) to the nasopharynx (the space behind the nose which communicates with the throat).  Coronal CT cisternogram showing CSF draining from the subarachnoid space through the roof of the right ethmoid sinus (arrow) into the nose.
Coronal CT cisternogram showing CSF draining from the subarachnoid space through the roof of the right ethmoid sinus (arrow) into the nose.  Coronal CT of a patient present with CSF rhinorrhea after ethmoid surgery. This non-contrast study shows a defect in the floor of the right ethmoid sinus and possible soft tissue or brain, filling this site (arrow).
Coronal CT of a patient present with CSF rhinorrhea after ethmoid surgery. This non-contrast study shows a defect in the floor of the right ethmoid sinus and possible soft tissue or brain, filling this site (arrow).  Coronal MRI of the patient on the left showing an encephalocele and CSF draining into the roof of the right ethmoid sinus (arrow). CSF is also visible as pooling within the maxillary sinus (MS).
Coronal MRI of the patient on the left showing an encephalocele and CSF draining into the roof of the right ethmoid sinus (arrow). CSF is also visible as pooling within the maxillary sinus (MS).  Coronal cadaver section illustrating various forms of repair of skull base defects. The three forms of grafting are the underlay, overlay and combined. In the underlay technique a graft (5) is placed on the under surface of the bony skull base (3). To improve adhesion of the graft to bone, the mucous membrane (4) is removed around the fistula site. In the overlay technique, the graft (2) is ideally placed between the dura (1) and the skull base (3). The third approach is to place two separate grafts, one as an overlay and the other as an underlay.
Coronal cadaver section illustrating various forms of repair of skull base defects. The three forms of grafting are the underlay, overlay and combined. In the underlay technique a graft (5) is placed on the under surface of the bony skull base (3). To improve adhesion of the graft to bone, the mucous membrane (4) is removed around the fistula site. In the overlay technique, the graft (2) is ideally placed between the dura (1) and the skull base (3). The third approach is to place two separate grafts, one as an overlay and the other as an underlay.  Intraoperative photograph of skull base defect through the brain (1) can be seen with the dura (2) and mucous membrane (3) of the ethmoid sinus in the foreground.
Intraoperative photograph of skull base defect through the brain (1) can be seen with the dura (2) and mucous membrane (3) of the ethmoid sinus in the foreground.  Abdominal fat graft (1) is shown being placed within the intracranial defect (2). When this step is completed, >80% of the fat graft is intracranial with only a small portion projecting through the dura into the nose. Fat works particularly well for such repairs because it “plugs” or fills the opening well and minimally shrinks over time.
Abdominal fat graft (1) is shown being placed within the intracranial defect (2). When this step is completed, >80% of the fat graft is intracranial with only a small portion projecting through the dura into the nose. Fat works particularly well for such repairs because it “plugs” or fills the opening well and minimally shrinks over time.  The next stage of the repair is placement of tissue glue (1) as defect site, and then adheres the second graft (2) to roof of the nose. The procedure is completed with the placement of absorbable packing against the intranasal graft.
The next stage of the repair is placement of tissue glue (1) as defect site, and then adheres the second graft (2) to roof of the nose. The procedure is completed with the placement of absorbable packing against the intranasal graft.  Coronal CT scan showing CSF pooling in the right sphenoid sinus secondary to a defect in the wall of this sinus. CSF fistulas into the sphenoid sinus are repaired using similar techniques and tissue grafting as described for the ethmoid sinus.
Coronal CT scan showing CSF pooling in the right sphenoid sinus secondary to a defect in the wall of this sinus. CSF fistulas into the sphenoid sinus are repaired using similar techniques and tissue grafting as described for the ethmoid sinus. 