| |
DISEASE STATES |
Section 5 of 10    |
|
|
CT scanning can be helpful in the diagnosis of acute and chronic sinusitis, neoplastic and inflammatory processes, and other problems (eg, congenital anomalies).
Acute sinusitis is caused by bacterial or fungal infections usually secondary to an obstructed sinus cavity. Structural anatomic variations, acute edema of sinonasal mucosa in response to infection or allergens, and compromise of nasociliary flow can all contribute to acute and chronic sinusitis. CT findings of sinus opacification, air-fluid levels, and thickened localized mucosa are all findings of acute sinusitis. Many nonspecific CT findings, including thickened turbinates (nasal cycle vs allergic process vs inflammation) or diffusely thickened sinus mucosa (allergic disease vs chronic sinusitis), may be associated with several sinonasal conditions.
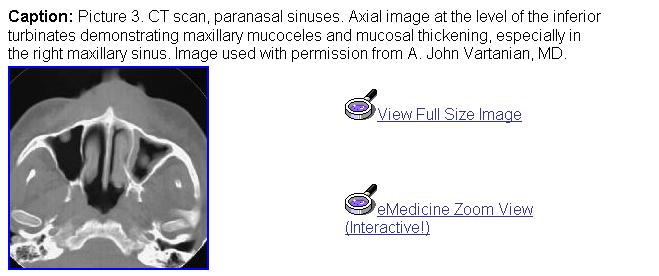
In chronic sinusitis, repeated episodes of acute sinusitis or festering infection usually combined with unfavorable anatomic factors lead to a vicious cycle of infection, mucociliary incompetence, and chronic mucosal inflammation. CT findings suggestive of chronic sinusitis include mucosal thickening, opacified air cells, bony remodeling, and bony thickening due to inflammatory osteitis of the sinus cavity walls. Bony erosion can occur in severe cases, especially if associated with massive polyps or mucoceles. CT findings of bony destruction should alert the clinician to also consider less common diseases, such as sinonasal tumors or granulomatous disease processes.
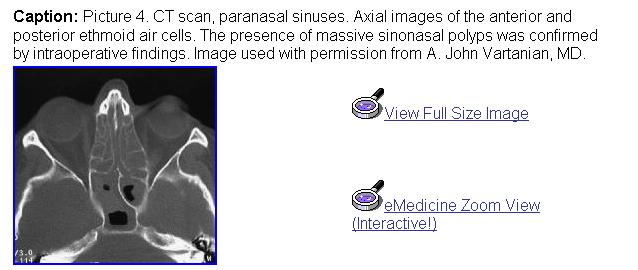
Sinonasal polyps can create sinus disease by obstruction or mass effect and by causing secondary infections. Sinonasal polyps appear on CT scans as nodular or rounded masses and amorphous opacified blobs of tissue. Bony remodeling can occur, but it is typically subtle, which is expected from the usual slow growth pattern of sinonasal polyps and benign processes in general.
Fungal sinusitis can be divided into invasive fungal sinusitis, chronic noninvasive fungal sinusitis (mycetoma), and allergic fungal sinusitis. Invasive fungal sinusitis due to mucormycosis or aspergillosis is typically a disease that affects immunocompromised patients and can have a fulminant course. Early in the disease process, opacification of sinuses is seen. Disease progression to a more fulminant state accompanies vascular invasion and localized destruction. Intracranial, cavernous sinus, and orbital complications may occur with advanced infections. CT findings mirror these processes with expanding localized destruction of bone.
Mycetomas appear inside the sinus cavity as noninvasive balls of fungus. CT findings may include a localized sinus opacification, homogenous mass that does not change shape with head position (gravity), and a mass with presence of calcifications (found in 25% of cases).
Allergic fungal sinusitis (AFS) may occur in atopic patients as a hypersensitivity reaction to fungal antigens. Many patients with AFS may also have various degrees of nasal polyposis. On CT scans, heterogeneous opacification can be seen with a typical pattern of central hyperdense areas of opacification surrounded by less dense areas of opacification. Calcified areas can sometimes be seen. Bony expansion, remodeling, and even diffuse bony destruction can be seen in advanced cases.
With experience, CT findings can be accurately correlated with anatomic and clinical realities of the particular patient. As for all radiologic surveys, sinus CT scans must be read with a systematic approach. After the primary survey of the CT scan is completed, including patient name, indications for the CT scan, type of scan, cross-sectional view being discussed, and major radiologic findings, particular attention is directed toward potential "bottle-neck" areas, where normal passages may be occluded by disease states or variant anatomy.
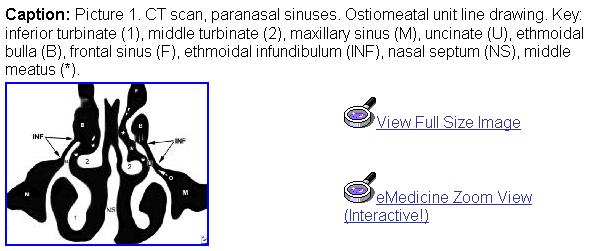
A systematic approach is helpful when interpreting CT scans. Reading the CT scan from anterior to posterior (on coronal views) or from top to bottom (on axial sections) can help organize one's approach in analyzing structures to be interpreted. For initial orientation, a number of important paranasal sinus structures are identified, including the frontal sinuses, the frontal recess, the agger nasi cells, the anterior ethmoidal sinus cells, the ethmoid roof, the ethmoidal bulla, the uncinate process, the ethmoidal infundibulum, the maxillary sinus, the middle meatus, the nasal septum, the turbinates, the basal lamella, the posterior and anterior ethmoid cells, and the sphenoid sinus.
If the CT scan is being read as a prelude to surgery, a number of additional anatomic and structural features need to be considered. The thickness, orientation, and most medial position of the lamina papyracea must be noted. Any dehiscences or excessive medial bowing of this thin bone should be noted prior to surgery. Similarly, the depth of the olfactory fossa must be recognized. The relationship of the sphenoid sinus and posterior ethmoid air cells vis a vis the internal carotid artery and optic nerves should be noted.
| |
IMPORTANT RADIOLOGIC ANATOMIC LANDMARKS |
Section 6 of 10 |
|
|
Landmarks on coronal CT sections
- Relationship of cells within the frontal recess and their relationship to the frontal sinuses
- Depth of the olfactory fossa: The deeper the fossa (ie, increased distance from the cribriform plate and the fovea ethmoidalis), the higher the chance for fracture or perforation with surgical maneuvers.
- Slope, thickness, and asymmetries in the height of the ethmoid roof
- The prevalence of intracranial penetration during FESS is higher when this anatomic variation occurs.
- Intracranial penetration is more likely to occur on the side with the lower roof.
- Patency of the ostiomeatal complex
- Attachment of the middle turbinate
- Width of the infundibulum
- Vertical distance from the maxillary sinus to the ethmoid roof in posterior ethmoid cells
- Degree of pneumatization of the maxillary sinus
- Status of the lamina papyracea
- Dehiscence in the lamina papyracea
- Shape of the medial orbital wall
- Attachment of the uncinate process
- Alignment of the septum
- Size and status of the maxillary sinuses (hypoplastic vs normal size)
- Other variations, such as the presence of a concha bullosa
Landmarks on axial CT sections
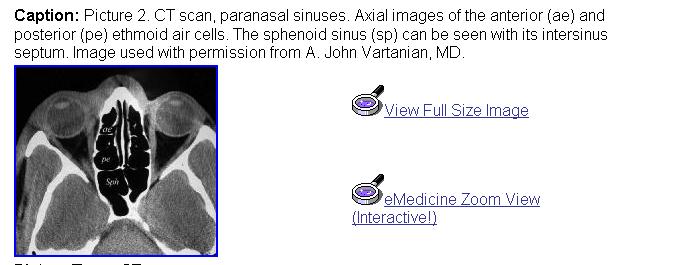
- Depth and ratio of the anterior and posterior ethmoid cells compared to the sphenoid sinus
- Degree of pneumatization of sphenoid sinus
- Position of sphenoid intersinus septae
- Presence or absence of an Onodi cell (sphenoethmoidal cell)
- Dehiscence in the bony covering of the carotid artery or optic nerve
- Relationship of the optic nerve to the posterior ethmoid cells
- The presence of anterior clinoid process pneumatization
- Degree of indentation created by the carotid artery and optic nerve
- Position of uncinate (medial versus lateral)
- Patency of the ostiomeatal complex
- Patency of the V-shaped ethmoidal infundibulum
- Alignment of the septum
| |
SUMMARY OF BASIC SINONASAL ANATOMIC TERMS |
Section 7 of 10 |
|
|
Agger nasi: This is a bony prominence that is often pneumatized in the ascending process of the maxilla. Its location below the frontal sinus also defines the anterior limit of the frontal recess.
Concha bullosa: The concha bullosa is a pneumatized middle turbinate. An enlarged middle turbinate may obstruct the middle meatus and the infundibulum causing recurrent disease. It may also serve as a focal area of sinus disease.
Ethmoidal bulla: This is the largest and most anterior ethmoid cell system. It is found posterior to the middle turbinate and posteromedial to the uncinate process.
Ethmoidal infundibulum: This is a space bordered medially by the uncinate process and laterally by the lamina papyracea. The maxillary sinus ostium is found inferiorly and laterally within this space.
Haller cell (infraorbital cell): The Haller cell is usually situated below the orbit in the roof of the maxillary sinus. It is a pneumatized ethmoid cell that projects along the medial roof of the maxillary sinus. Enlarged Haller cells may contribute to narrowing of the ethmoidal infundibulum and recurrent sinus disease, despite previous (incomplete) surgery.
Frontal recess: This is an hourglass-shaped space between the inferomedial aspect of the frontal sinus and the anterior middle meatus. Unfavorable variations of the structures that define its borders may cause problems with the frontal sinus outflow tract. These structures include the agger nasi cell, supraorbital ethmoid cells, the ethmoid bulla, and inferiorly, the uncinate process.
Lamina papyracea: This is a thin, bony wall separating the orbit from the ethmoid air cells. Dehiscences may occur for congenital reasons or because of previous surgery or facial trauma.
Maxillary sinus ostium: This is the opening of the maxillary sinus to the nasal cavity and a part of the ostiomeatal complex.
Ostiomeatal complex or unit: This term refers to a collection of middle meatal structures and is not a discrete anatomic entity. It consists of the ethmoid infundibulum, anterior ethmoid cells, and the uncinate process. It also represents the final common pathway of drainage for the frontal, maxillary, and anterior ethmoid cells. A patent ostiomeatal complex is essential for the improvement of patients with sinus disease.
Paradoxical middle turbinate: The major curvature of the middle turbinate may project laterally, leading to narrowing of the middle meatus.
Sphenoethmoid cell (Onodi cell): This is formed by lateral and posterior pneumatization of the most posterior ethmoid cells over the sphenoid sinus. The presence of Onodi cells increases the chance that the optic nerve and/or carotid artery would be exposed (or nearly exposed) in the pneumatized cell.
Uncinate process: This is a 3-dimensional sickle-shaped (also described as a hook- or L-shaped) bone of the lateral nasal wall. Anteriorly, the uncinate process attaches to the lacrimal bone; inferiorly, the uncinate process attaches to the ethmoidal process of the inferior turbinate. The posterior edge lies in the hiatus semilunaris inferioris. Superiorly, the uncinate process may attach to the middle turbinate, lamina papyracea, and/or the skull base.
- In general, the larger the air cells, the thinner the bony walls become. This may increase the chance for injuring structures within or adjacent to such bony structures lining the air cell.
- On CT scan, AFS is depicted as a heterogenous opacification that can be seen with a typical pattern of central hyperdense areas of opacification surrounded by less dense areas of opacification.
- Unilateral sinonasal polypoid soft tissue masses in the area of the ethmoid cells may represent a herniated encephalocele. An MRI may be helpful in its differentiation.
|